Here are some thoughts about what is/was going on in our floxed bodies.
First, here’s my typical disclaimer. I’m not a doctor or scientist. I’m doing my best to put together this information, but I could be wrong. I do my best to be right and I back up my assertions with peer-reviewed journal articles.
As I mentioned in Article Breakdown – “Mechanisms of Pathogenesis in Drug Hepatotoxicity Putting the Stress on Mitochondria,” I believe that this paragraph describes much of what occurs in floxed cells:
“Increased steady-state levels of mitochondrial superoxide, arising from reduction of Sod2 activity in the Sod+/−mice (i.e., approximately half the wild-type activity), may be exacerbated by drugs that directly target the ETC [e.g., the complex I inhibitors flutamide and troglitazone (122)]. The increased amount of superoxide raises two considerations. First, superoxide that escapes dismutation to hydrogen peroxide cannot cross the inner mitochondrial membrane and can oxidize [Fe-S]-containing enzymes (e.g., aconitase and complex I/III subunits). Alternatively, superoxide can rapidly react with mitochondrial nitric oxide (NO) to form peroxynitrite (ONOO−). For example, the fluoroquinolone antibiotic trovafloxacin (TVX), a typical DILI (drug induced liver injury) associated drug, raises steady-state levels of NO in hepatocellular mitochondria (unpublished data). The mechanisms are not known, but TVX also increases cytosolic (non-ferritin-bound) Ca2+, likely activating the Ca2+-dependent mitochondrial NO synthase (123) to produce ONOO−. Peroxynitrite is dangerous for a number of reasons: i) under acidic conditions, it can be degraded to form the extremely reactive hydroxyl radical; ii) it may directly cause the nitration of aconitase, Sod2, and the [Fe-S]-containing subunits of ETC complexes; and iii) it can induce mitochondrial permeabilization (Figure 4B) (124). This superimposed oxidative/nitrative stress could ultimately push the cell across the threshold to observable injury.”
SUPEROXIDE DAMAGE OF MITOCHONDRIAL DNA
Superoxide is a powerful oxidant that is quite toxic. Per “Mitochondrial matrix reactive oxygen species production is very sensitive to mild uncoupling,” “ROS are produced continuously as a by-product of aerobic metabolism. Superoxide can be produced as a result of the one-electron reduction system within the mitochondrial electron transport chain. Superoxide can then be converted into hydrogen peroxide (H2O2) by superoxide dismutase (the Mn isoform in the matrix and cu, Zn-superoxide dismutase in the cytosol). H2O2 can be converted into highly reactive hydroxyl radicals (OH-) by the Fenton reaction, and can cause lipid peroxidation.” More info about superoxide can be found here – http://en.wikipedia.org/wiki/Superoxide
In properly functioning cells, superoxide dismutase (SOD) converts superoxide into hydrogen peroxide (H2O2) and water. Unfortunately, fluoroquinolones deplete cellular SOD. In “Oxidative Stress Induced by Fluoroquinolones on Treatment for Complicated Urinary Tract Infections in Indian Patients” it was found that, for human patients with urinary tract infections and treated with various fluoroquinolones, “There was substantial depletion in both SOD and glutathione levels particularly with ciprofloxacin.”
Without sufficient SOD, as noted above, superoxide “cannot cross the inner mitochondrial membrane and can oxidize.” Oxidization within the mitochondrial membrane is harmful because it damages mitochondrial DNA (mtDNA) and starts the vicious cycle of oxidative damage to mitochondria. (This “vicious cycle” theory is described in “Oxidative stress induces degradation of mitochondrial DNA” – “According to this theory, the production of ROS by mitochondria leads to mtDNA damage and mutations which in turn lead to progressive respiratory chain dysfunction and to a further increase in ROS production as a consequence of this dysfunction. The exponential escalation of these processes is commonly referred to as a ‘vicious cycle’, and the theory predicts that the rise in mtDNA mutations and ROS eventually reach levels that are incompatible with life.” It should be noted that whether or not this theory is true for how aging works is contentious. The vicious cycle of damage done by ROS does occur in mitochondria though.)
THE NITRIC OXIDE / PEROXYNITRITE (NO/ONOO-) CYCLE
Additionally, “superoxide can rapidly react with mitochondrial nitric oxide (NO) to form peroxynitrite (ONOO−).” The ways in which peroxynitrite are dangerous are noted in the paragraph from “Mechanisms of Pathogenesis” at the beginning of this post.
Dr. Martin L. Pall, Professor Emeritus of Biochemistry and Basic Medical Sciences at Washington State University describes the NO/ONOO- (nitric oxide / peroxynitrite) cycle in his web site, http://www.thetenthparadigm.org/index.html. Here is a diagram from The Tenth Paradigm describing the NO/ONOO- cycle –
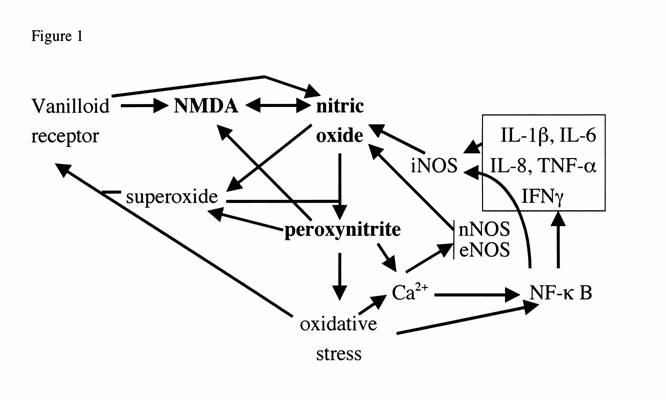
Here is Dr. Pall’s description of the above diagram:
“Fig. 1 legend. Vicious (NO/ONOO-) cycle diagram. Each arrow represents one or more mechanisms by which the variable at the foot of the arrow can stimulate the level of the variable at the head of the arrow. It can be seen that these arrows form a series of loops that can potentially continue to stimulate each other. An example of this would be that nitric oxide can increase peroxynitrite which can stimulate oxidative stress which can stimulate NF-kappaB which can increase the production of iNOS which can, in turn increase nitric oxide. This loop alone constitutes a potential vicious cycle and there are a number of other loops, diagrammed in the figure that can collectively make up a much larger vicious cycle. The challenge, according to this view, in these illnesses is to lower this whole pattern of elevations to get back into a normal range. You will note that the cycle not only includes the compounds nitric oxide, superoxide and peroxynitrite but a series of other elements, including the transcription factor NF-kappaB, oxidative stress, inflammatory cytokines (in box, upper right), the three different forms of the enzymes that make nitric oxide (the nitric oxide synthases iNOS, nNOS and eNOS), and two neurological receptors the vanilloid (TRPV1) receptor and the NMDA receptor.”
The NO/ONOO- cycle provides a reasonable explanation for why it feels as if a bomb has gone off in the body of the floxie. It also is an explanation as to why the adverse effects of drugs that damage mitochondria and cause oxidative stress are not transient. There are feedback loops within the cells that perpetuate the damage.
Here is Dr. Pall’s table of signs of the NO/ONOO- cycle –
Explanations for Symptoms and Signs
| Symptom/Sign | Explanation based on elevated nitric oxide/peroxynitrite theory |
| energy metabolism /mitochondrial dysfunction | Inactivation of several proteins in the mitochondrion by peroxynitrite; inhibition of some mitochondrial enzymes by nitric oxide and superoxide |
| oxidative stress | Peroxynitrite, superoxide and other oxidants |
| PET scan changes | Energy metabolism dysfunction leading to change transport of probe; changes in perfusion by nitric oxide, peroxynitrite and isoprostanes |
| SPECT scan changes | Depletion of reduced glutathione by oxidative stress; perfusion changes as under PET scan changes |
| Low NK cell function | Superoxide and other oxidants acting to lower NK cell function |
| Elevated cytokines | NF-kappaB stimulating of the activity of inflammatory cytokine genes |
| Anxiety | Excessive NMDA activity in the amygdala |
| Depression | Elevated nitric oxide leading to depression; cytokines and NMDA increases acting in part or in whole via nitric oxide. |
| Rage | Excessive NMDA activity in the periaqueductal gray region of the midbrain |
| Cognitive/learning and memory dysfunction | Lowered energy metabolism in the brain, which is very susceptible to such changes; excessive NMDA activity and nitric oxide levels and their effects of learning and memory |
| Multiorgan pain | All components of cycle have a role, acting in part through nitric oxide and cyclic GMP elevation |
| Fatigue | Energy metabolism dysfunction |
| Sleep disturbance | Sleep impacted by inflammatory cytokines, NF-kappaB activity and nitric oxide |
| Orthostatic intolerance | Two mechanisms: Nitric oxide-mediated vasodilation leading to blood pooling in the lower body; nitric oxide-mediated sympathetic nervous system dysfunction |
| Irritable bowel syndrome | Sensitivity and other changes produced by excessive vanilloid and NMDA activity, increased nitric oxide |
| Intestinal permeabilization leading to food allergies | Permeabilization produced by excessive nitric oxide, inflammatory cytokines, NF-kappaB activity and peroxynitrite; peroxynitrite acts in part by stimulating poly ADP-ribose polymerase activity |
Sounds pretty familiar, doesn’t it?
STOPPING THE NO/ONOO- CYCLE
What can be done to stop the NO/ONOO- cycle? How can one heal when cells are reinforcing the damage done to them over and over again?
Here are Dr. Pall’s recommendations – http://www.thetenthparadigm.org/therapy.htm
Additionally, a very smart and appreciated floxie noted in a comment on this site, that uric acid has been shown to decrease peroxynitrite. Per the article, “Uric acid, a natural scavenger of peroxynitrite, in experimental allergic encephalomyelitis and multiple sclerosis,” “Uric acid, the naturally occurring product of purine metabolism, is a strong peroxynitrite scavenger, as demonstrated by the capacity to bind peroxynitrite but not nitric oxide (NO).” (There has been some debate about whether floxies want to increase or decrease nitric oxide. I think that we want to increase NO because too much of it is converted into peroxynitrite. Here’s an article on how NO helps with tendon healing – “The role of nitric oxide in tendon healing.”) Uric acid. The stuff that causes kidney stones and gout – it’s a powerful antioxidant that scavenges peroxynitrite.
The role that uric acid plays in getting rid of toxic peroxynitrite makes sense to me on a personal level because of a couple of things that have made me feel significantly better post-flox – brewer’s yeast and uridine supplements. Both brewer’s yeast and uridine are high in purines, which are converted into uric acid in the body. I always thought that the purines and uric acid were a necessary evil and that the good done by brewer’s yeast had to do with its high amino acid and/or B vitamin content. Now I’m thinking that the necessary evil was actually the active ingredient.

Here are a couple more articles about the role of uric acid in peroxynitrite neutralization (thanks again to the floxie friend who pointed them out):
- “A reassessment of the peroxynitrite scavenging activity of uric acid.”
- “Interactions of peroxynitrite with uric acid in the presence of ascorbate and thiols: implications for uncoupling endothelial nitric oxide synthase.”
- “Nitrosation of Uric Acid by Peroxynitrite: FORMATION OF A VASOACTIVE NITRIC OXIDE DONOR”
There is a very real risk of kidney stones and gout when consuming too many purines that lead to excess uric acid. Even though brewer’s yeast has helped me immensely, I feel quite conflicted about it. I don’t want a kidney stone and gout would probably make my flox-induced peripheral neuropathy look like a cake-walk. Now that I’m feeling well, I’m probably going to cut way down on my brewer’s yeast consumption. I really don’t know which are worse – the diseases of too much uric acid (kidney stones and gout) or the diseases of too little uric acid (“patients with MS have significantly lower levels of serum uric acid than controls” and peroxynitrite is associated with lots of other nasty diseases – like cancer and Alzheimer’s). This isn’t exactly a great predicament.
Another consideration is that fluoroquinolones deplete cellular magnesium and proper amounts of cellular magnesium are necessary for 300+ enzymatic reactions. (Fluoroquinolones may inhibit and deplete enzymes through means other than depletion of cellular magnesium too.) If one doesn’t have the enzymes to metabolize uric acid, well, too much isn’t a good thing. Too much peroxynitrite is bad too though.
I wish that the answers were more clear. I hope that this post at least gave you some information with which you can make an informed decision!
In researching this post, I stumbled upon this interesting web site – http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/R/ROS.html It is noted on the site that uric acid is an antioxidant and that, “Perhaps the long life span of some reptiles and birds is attributable to their high levels of uric acid.” Bird shit and reptile blood are full of the stuff. If there is a cure for fluoroquinolone toxicity, it’ll probably come from bird turds or alligator blood. Great.








{kind=link}
At least I understood that last paragraph and even got a chuckle! The rest is way over my head at this point.
Very interesting article.I had a PET scan after I have been floxed and it said I have glucose metabolism proplems.That is a energy matabolism problem as said in the article, since glucose is the brain’s fuel.
So would a super oxide dismutase supplement + CoQ10 + PQQ + some other antioxidants like Acai berry (if IV glutathion is not available for me) be helpful ?
A couple of observations…excellent article by the way.
In your article you state something very critical… “There are feedback loops within the cells that perpetuate the damage”, this is so very true.
I have vigorously debated the NO conundrum, with myself over the last few years as I have definite signs of a very dysfunctional NO/ONOO cycle. I am currently experimenting, with the help of my talented person physician, in trying to increase NO levels during times that I experience pain and inflammation to see if it helps. We are using glyceryl trinitrate in two different delivery mechanisms.
For what its worth…last year I induced a case of gout by taking some molybdenum while I was eating some fresh lentil soup. I have never had gout nor do I have any hereditary predisposition to it. Other than hobbling around with an extremely sore big toe and foot, the rest of me felt pretty good. Hmmmmm
Keep of the good work!
Any idea why my tendon symptoms (only symptoms) came on 2 wks post cipro, after by chance taking pycogenol for 4 days, as it is a super antioxidant?
Also does this stop at some point post floxing or is it forever? On last thing, was hoping that article might clarify what best to take for multi tendon stuff, any key top 5 suggestions? May thanks for this site it has been the only light of hope amongst much misery! Thank you
Thank you for the reply.
So to stop the vicious cycle with antioxidants? …which would be best for that? I did read the piece twice but twice it went over my head.
(continued)
There’s a comment above about molybdenum. I can also say in large doses (~1g) it has a noticeable mental effect on me for whatever reason. I also took about 500mcg for 1-2 months at some point.
I can also say (although I’m having problems at the moment) I didn’t really have serious relapses since the FQ, and most of the time I was eating another high source of purines. The times I wasn’t eating it, I was getting more fructose, which can also raise uric acid. Also that molybdenum now that it’s been mentioned. I have bad problems at the moment (hence slow replies) but I don’t think they’re FQ-mito-damage-related; unrelated trigger.
Maybe the takeaway for uric acid is to avoid being too low in it, maybe increase it in periods of stress. It seems like a fairly natural method, because when you look at the high-purine foods they’re very paleo. I’m not so much afraid of gout (I think probably fruit are preventative) as the possibility of uric acid crystals in joints.
I never found anything too helpful regarding superoxide dismutase (SOD1, SOD2, SOD3). There are liposomal SOD1 supplements but from what I understood they wouldn’t help if SOD2 activity is affected. The only thing I do is try to get enough manganese, since SOD2 relies it and there’s some research articles where it partly compensates (but for SOD1? I don’t know). Also zinc/copper for SOD1 but lack of testing means I have to back off. As a footnote, is some people do better on vegetarian diets; these are usually higher in manganese. Tendons also need it. Also somebody mentioned Pycnogenol above, I think there are studies that link it to improving SOD.
What I took away from the first article in the bullet list (“A reassessment […]”) is not to take baking soda for too long (I did this for awhile too but not in athletic amounts). But that’s not news.
One thing I haven’t tried is supplementing with BH4 directly, because it’s too expensive. I do the other suggestions, methylfolate, vit C, niacin, etc. instead, plus leafy greens, now sunlight and consciously uric acid, etc. Major conflict that comes up is that one of the suggestions to help BH4 is to limit protein, to help with ammonia and limit BH4 use, but you very much need protein for tendons and tons else.
Anyway I’m out of breath but great article, sorry if I missed something.
Both Lou and Impossibleadversity,
THANK YOU so much for the insights, information and the really interesting conversation! I need to look more thoroughly into both of your comments, but here are some initial thoughts.
I don’t think that the reaction is linear. Non-linear reactions are confusing as hell – to say the least. I suspect that there are adaptive responses that occur in cells that are actually healthy and good when those cells are exposed to harm. It is only after the harm threshold is crossed that both harm is done and it is perpetuated within the cell. I also suspect that each floxie’s reaction to supplements (and other things – like drugs) depends on what stage of harm the cells are in. Severely damaged cells react differently to antioxidant supplements than moderately damaged cells. I think that’s why some people have a paradoxical reaction to antioxidant supplements that help most floxies.
I honestly need to do more research to confirm or disprove these notions. But those are my thoughts.
Lisa
Impossible diversity, is that to say doxycycline can fix this mess?? No nothings that simple, can you explain it in laymens what doxy can do and how lasting? …As by chance I have some in my cupboard 😀
You were also taking pycogenol and the same happened to you… STOP now I carried on a while, not good.
Here’s another interesting article: https://www.lef.org/protocols/immune_connective_joint/gout_01.htm
One of the most intriguing aspects of uric acid is that although it appears to be a “waste product” of purine metabolism, only about 10% of the uric acid that enters a normal human kidney is excreted from the body (Richette 2010). In other words, rather than eliminating uric acid, a healthy kidney returns up to 90% of it to the blood stream. The reason for this is likely due to the role or uric acid as one of the most important antioxidants in body fluids, responsible for the neutralization of over 50% of the free radicals in the blood stream (Glantzounis 2005).
The ability of humans and primates to preserve blood levels of uric acid (due to slow kidney filtration and lack of a uricase enzyme) was probably advantageous to our evolution, by increasing antioxidant capacity of the blood (Alvarez-Lario and Macarrón-Vicente 2011).
Humans and primates are one of the few mammals that cannot produce their own vitamin C, and may have evolved the ability to preserve uric acid to compensate for this (Hediger 2002). For example, blood uric acid levels in humans are normally about 6 times that of vitamin C, and about ten times the levels in other mammals (Roch-Ramel 1999). Like vitamin C, uric acid has a principle role in protecting high-oxygen tissues (like the brain) from damage, and low blood uric acid levels have been associated with the progression or increased risk of several neurological disorders, including Amyotrophic Lateral Sclerosis (Keizmann 2009), Multiple sclerosis (Rentzos 2006), and Huntington’s (Auinger 2010), Parkinson’s (Andreadou 2009), and Alzheimer’s diseases (Kim 2006).
That said I too have concerns about it at the moment.
Fascinating! Thank you so much for posting! I wish that it was a pure good and was inconsequential though. My left flank hurts and I’m wondering if it’s a kidney stone. I sure hope not. I’m laying off of the brewer’s yeast for a bit – at least until I feel better.
Jigsaw but fascinating I agree.
Lisa I wonder if a high purine diet would be part of the key then… http://www.mayoclinic.org/healthy-living/nutrition-and-healthy-eating/in-depth/gout-diet/art-20048524
Are floxies more likely to get gout than any other group? Or are you just worried about getting gout in general, from the high purine diet?
Impossible adversity, does this contradict? Early morning in UK, hard to comprehend Doxy idea 🙂 : http://www.ncbi.nlm.nih.gov/pubmed/17260615
OK am waking up, this is REALLY interesting esp the discussion section on tendon repair.http://www.ors.org/Transactions/55/1421.pdf
Great comments! Google L-Ornithine, urea cycle, Dr David Jernigan. Helped me a lot!
Probably worth posting: The recommended max amount of daily purine from foods is supposedly about 1800mg/day: http://librariannihilation.wordpress.com/2008/10/02/maximum-daily-allowance/
There is also a google book that recommends 2000mg/day max (lost link).
what about IV C and IV glutathione. they are antioxidants. why some floxies (me too) get herxes after taking them?