
I’m so excited to share this article, “Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications” by Krzysztof Michalak, Aleksandra Sobolewska-Wlodarczyk, Marcin Włodarczyk, Justyna Sobolewska, Piotr Woźniak, and Bogusław Sobolewski, with you! It is the first article of its kind that I’ve seen. While there are thousands of articles about fluoroquinolones, many of which focus on the damaging effects of fluoroquinolones, and many case-studies that note the adverse-effects of fluoroquinolones (hundreds of articles about fluoroquinolones are linked HERE), this is the first article that acknowledges that fluoroquinolone toxicity (referred to as both Fluoroquinolone Associated Disability (FQAD) and fluoroquinolone toxicity throughout the article) is a disabling syndrome, that also goes over the mechanisms by which fluoroquinolones can cause fluoroquinolone toxicity/FQAD, and even gives recommendations on how to treat fluoroquinolone toxicity/FQAD (while also acknowledging that there are no cures or verified treatments). The article even calls for more extensive research to be done into fluoroquinolone toxicity, and the various mechanisms through which fluoroquinolones hurt people.
It is an enlightening article, and I encourage you to print it out and give it to your doctors, family members, and anyone else who is interested in what fluoroquinolones do and how they hurt people. In this post, I’m going to go over some highlights from the article, but I recommend that you read it yourself (you can access it through THIS LINK, after clicking on the “provisional pdf” link).
The first paragraph of the abstract to the article states:
“Long term Fluoroquinolone Associated Disability (FQAD) after fluoroquinolone (FQ) antibiotic therapy appears in recent years a significant medical and social problem, because patients suffer for many years after prescribed antimicrobial FQ-treatment from tiredness, concentration problems, neuropathies, tendinopathies and other symptoms. The knowledge about the molecular activity of FQs in the cells remains unclear in many details. The effective treatment of this chronic state remains difficult and not effective. The current paper reviews the pathobiochemical properties of FQs, hints the directions for further research and reviews the research concerning the proposed treatment of patients.”
To see that in writing, in an academic article, is incredibly validating.
Adverse Effects of Fluoroquinolones
Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications, goes over the documented effects of fluoroquinolones. For tendinopathies and tendon ruptures, researchers have found that:
“FQs are associated with an increased risk of tendinitis and tendon rupture. This risk is further increased in those over age 60, in kidney, heart, and lung transplant recipients, and with use of concomitant steroid therapy.”
Fluoroquinolones cause neurotoxicity, as well as central and peripheral nervous system ailments:
“Taking FQs is associated with their neurotoxicity, as well [5-8]. The main symptoms being correlated to FQ treatment include insomnia, restlessness, and rarely, seizure, convulsions, and psychosis [9-11]. Many reports point to chronic persistent peripheral neuropathy to be generated by FQs [12-18]. Cohen et al. [19] showed that a possible association between FQ and severe, long-term adverse effects involving the peripheral nervous system as well as other organ systems are observed.
Fluoroquinolones also cause cardiotoxicity and an elongation of the QT interval, as well as hepatotoxicity and nephrotoxicity. Fluoroquinolone use has even been linked to type-2 diabetes onset.
Fluoroquinolone toxicity / FQAD is a multi-symptom, chronic illness that affects all body systems. Fluoroquinolones deleteriously affect every muscle, tendon, ligament, nerve, and even bone, in the body. They damage every cell in the body.
Fluoroquinolone Damage Mechanisms
Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications, notes the various mechanisms by which fluoroquinolones cause cellular (mitochondrial) damage, including oxidative stress, and the downstream effects of oxidative stress, including disruptions in the mitochondrial Permeability Transition Pore (PTP) (and the article authors state, “The influence of FQs on the detailed regulation of PTP is the urgent topic for further research.”), Calcium and magnesium homeostasis, lowered ATP production, and more.
Here is a diagram of the mechanisms of fluoroquinolone toxicity (published in the article):
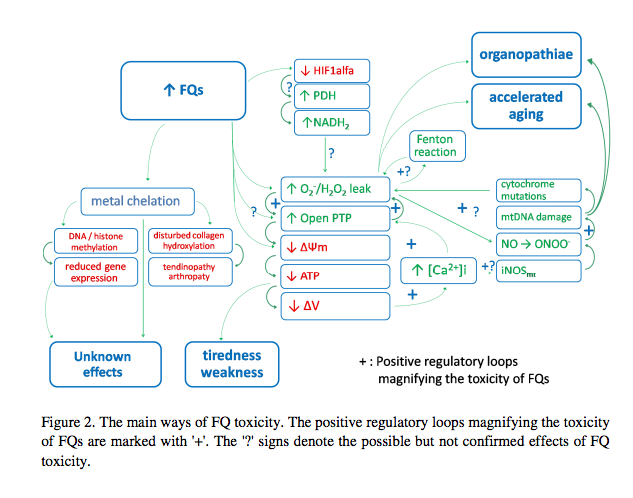
Figure 2. The main ways of FQ toxicity. The positive regulatory loops magnifying the toxicity of FQs are marked with ‘+’. The ‘?’ signs denote the possible but not confirmed effects of FQ toxicity.
The article also notes the epigenetic effects of fluoroquinolones and oxidative stress:
“Beside OS (oxidative stress), epigenetic effects of FQs are of high importance, as well. The epigenetic effects may depend on the methylation of DNA and/or histones, however, ROS contribute also to epigenetic changes [42]. Some authors point also to the similarity of bacterial and mitochondrial DNA, both existing in circular super-twisted helices and gyrase-like enzymes being postulated to be responsible for the organization of mitochondrial DNA, suggesting the possible direct effect of FQs to mitochondrial DNA leading to the disturbed mitochondria regeneration and division [43, 44]. The changes in the cytoskeleton were observed also after FQ treatment [45] and cytoskeleton has been demonstrated to be strictly connected with energy dissipation and organization in mitochondria [46-49].”
Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications, also notes that fluoroquinolones chelate various minerals and metals. The article notes that, “Seedher’s results indicate that chelation formation with bivalent metals can cause significant alterations in the human serum-FQ binding affinity.” The article also describes how fluoroquinolones chelate iron, zinc, magnesium, and other minerals, and how this chelation can have enzymatic and even epigenetic adverse effects.
Fluoroquinolones are GABA antagonists, and the effects of fluoroquinolones are similar to those of benzodiazepine withdrawal. The authors of Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications, describe a potential mechanism through which GABA is depleted by fluoroquinolones:
“One of the proteins which can support PTP opening is Translator Protein (TSPO), called also peripheral-type benzodiazepine receptor or isoquinoline binding protein. TSPO is predominantly located on the surface of the mitochondria where it is postulated to physically associate with VDAC-ANT. It has been suggested that TSPO may activate PTP opening, causing ∆Ψm reduction and leading to apoptosis [80, 81]. Some authors suggest that epileptogenic activity of FQs possibly relates to GABA-like structure of some FQs which may allow them to act as GABA antagonists [82, 83]. Since TSPO is also a benzodiazepine receptor, similar interaction may maybe also take place between FQs and TSPO leading to opening PTP.”
I have always wondered how GABA inhibition is connected to mitochondrial destruction. The article excerpt above answers that question for me.
Fluoroquinolones can lead to chronic illness and permanent disability, which has led many people to question whether or not they remain in the body for an extended period of time (or, if they do damage while they’re in the body that continues long after the drug has left the body). The authors of Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications note that:
“The other important feature of FQs has been presented by V.T. Andrioleet al. [55]. Namely, they estimated the minimum solubility of FQs in neutral pH. They pointed that this class of molecules is characterized by very high melting point, generally >200°C, which indicates that the crystal forms are very stable. All these FQ features strongly support the thesis that FQs can survive in the cell for a long time contributing to chronic, long-term adverse reaction in patients treated with FQs. The question, to what extent takes this phenomenon place and if it contributes to chronic symptoms of FQAD, remains unclear.”
It is acknowledged throughout the article that it is unknown whether or not fluoroquinolones stay in the body for an extended period of time. It is possible, through the mechanism noted above, but no hypotheses about fluoroquinolones remaining in the body after they “should” have been metabolized and fully excreted, have been explored. It’s both possible that they remain in cells, and that they don’t – no one really knows.
The article authors repeatedly call for additional research into the various mechanisms by which fluoroquinolones lead to pain, disability, and chronic illness:
“Summing up, the number of enzymes possessing reduced activity due to their ion-cofactor chelation is probably long and it is the important topic for further research. The separate problem consists the chronicity of ion-chelation by FQs. The presented research does not describe the chronic state of FQAD but the phenomena taking place during FQ application. It must be analyzed, to which degree persistent ion chelation takes place at FQAD patients.”
Fluoroquinolone Toxicity Treatment
Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications is the first article I’ve seen that discusses the treatment of fluoroquinolone toxicity as a multi-symptom, chronic illness. The authors note that the first step in approaching a treatment is to discover why fluoroquinolones are causing chronic illness in the first place. Effective treatment, of course, depends on effective identification of the problem. With that noted, the article authors have enough knowledge to make a few suggestions:
“Until detailed knowledge concerning FQ toxicity would be recognized, the following directions in supporting FQAD patients are proposed according to the known and probable mechanisms of FQ toxicity: A. reduction of the oxidative stress; B. restoring reduced mitochondrial potential ∆Ψm; C. supplementation of uni- and bivalent cations that are chelated by FQs;D. supporting the mitochondrial replication in the cell – pulling the more destroyed to apoptosis and proliferation of the more healthy ones; E. removing FQs permanently accumulated in the cells (if this phenomenon takes place); F. regulating the disturbed epigenetics and enzyme activities”
The article authors note that antioxidant supplementation is a broad topic and that fixing the damage done by fluoroquinolones and oxidative stress is not as simple as just ingesting an antioxidant pill. However, antioxidant supplements that specifically target the mitochondria have shown some promising results:
“The antioxidants which enter easily the mitochondria are the most interesting ones. Lowes et al. [79] shows that the mitochondria targeted antioxidant MitoQ protects against fluoroquinolone-induced oxidative stress and mitochondrial membrane damage in human Achilles tendon cells. In cells treated with MitoQ the oxidative stress was lower and mitochondrial membrane potential was maintained.”
Other antioxidants have also had promising results in repairing fluoroquinolone treated cells. Some of the antioxidants with promising results include N-acetylcysteine, resveratrol, as well as Vitamins C and E. Supplementation of the trace minerals that are important cofactors for antioxidants is also important.
Conclusion
I greatly appreciate the authors of Treatment of the Fluoroquinolone Associated Disability – the pathobiochemical implications. They approach fluoroquinolone toxicity/FQAD as a complex and multifaceted illness. It IS a complex and multifaceted illness, and it is refreshing to read an article that doesn’t over-simplify or downplay the illness. I also appreciate the exploration of what is currently known about fluoroquinolone toxicity/FQAD, and the assertions that more research into fluoroquinolone toxicity is needed (it is!). I think that everyone who is going through fluoroquinolone toxicity/FQAD should read it, and share it as widely as possible.










{kind=link}
… [Trackback]
[…] Find More to that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Read More to that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Read More here on that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] There you will find 46066 additional Information on that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Info to that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Find More Info here to that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Read More here on that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Find More on that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Find More to that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]
… [Trackback]
[…] Information on that Topic: floxiehope.com/fluoroquinolone-toxicity-article-treatment-of-the-fluoroquinolone-associated-disability-the-pathobiochemical-implications/ […]